Respiratory compromise is the major cause of morbidity and mortality in SMA. Individuals with SMA may have decreased respiratory function, underdeveloped lungs, and difficulty coughing and clearing secretions.1,2
In a study of individuals (n=49) with infantile-onset (Type I) SMA, those receiving early proactive noninvasive respiratory care did better compared with those treated with supportive respiratory care4
Children with SMA demonstrate a wide range of respiratory compromise3
Respiratory compromise in children with infantile-onset (consistent with Type I) SMA may be differentiated into 3 categories:3
Infants ≤5 months of age who require both continuous ventilatory support and non-oral nutritional support
Infants with ineffective cough who develop acute respiratory compromise during upper respiratory tract infections and require non-oral nutritional support before 24 months of age
Infants who do not develop respiratory compromise or who do not require non-oral nutritional support until after 24 months of age (approximately 10% of all children with infantile-onset SMA)
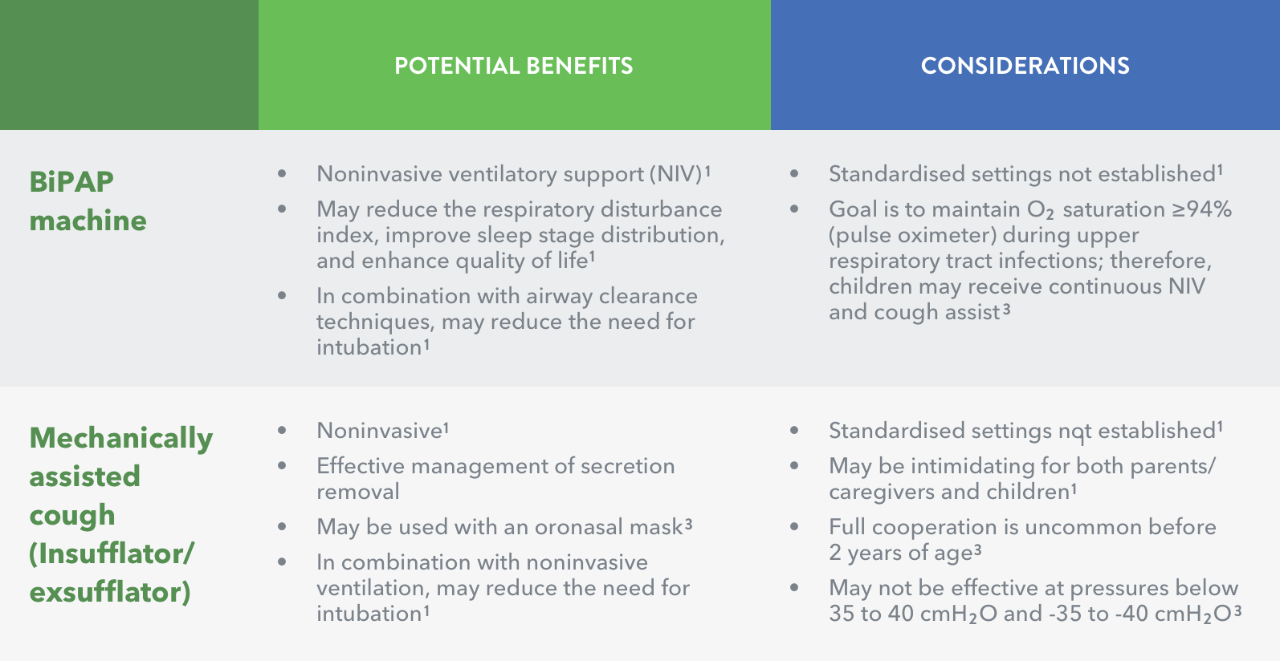
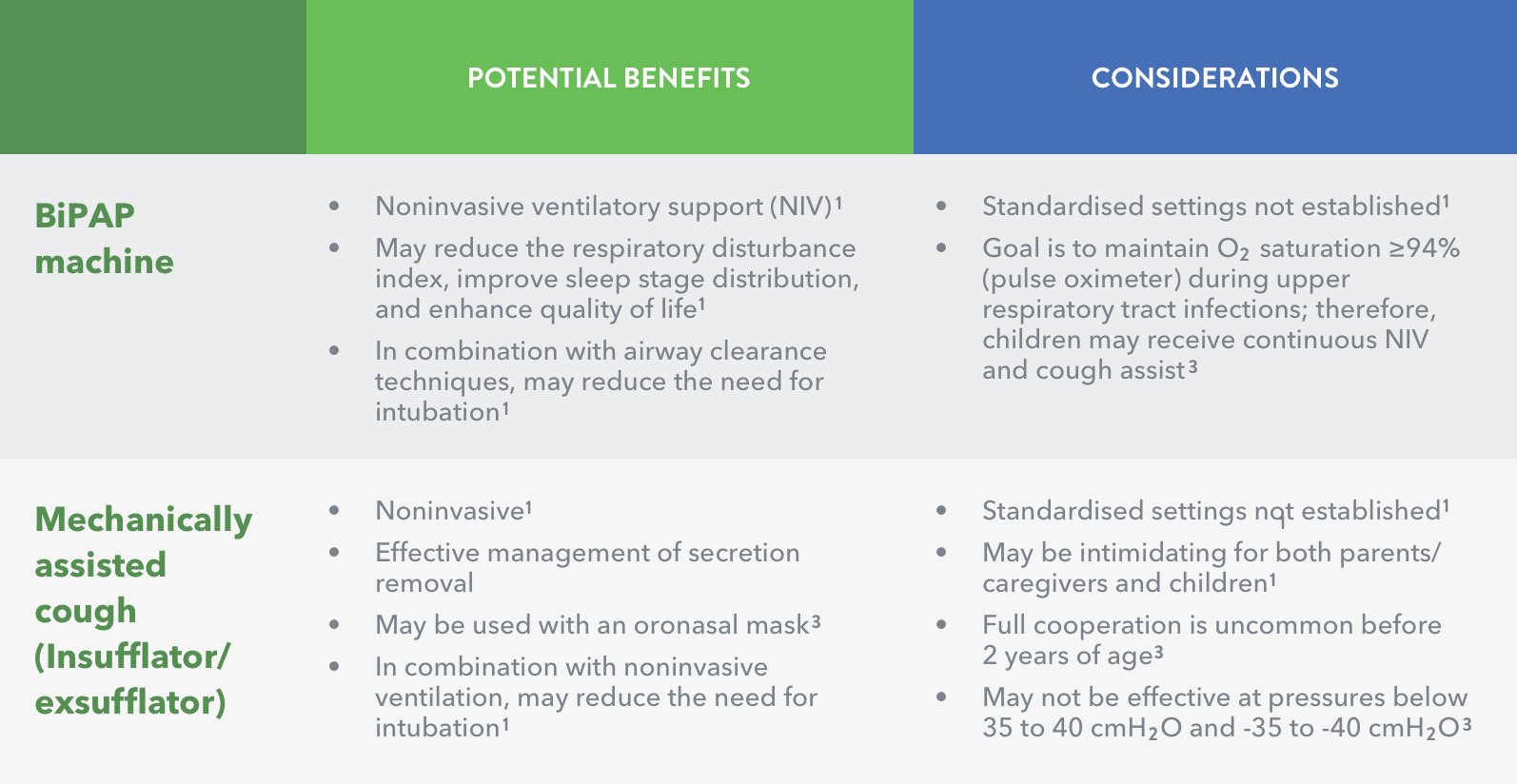
Noninvasive ventilatory support can be provided in the home2
Early proactive respiratory care was defined as:4
use of noninvasive bi-level positive airway pressure (BiPAP) at night and during daytime sleep, and
cough-assist device used at least twice-daily, initiated in the first 3 months after diagnosis.
Supportive care was defined as:4
other respiratory support, such as supplemental oxygen and suctioning.
Since the mid-1990s, three main areas of development have occurred in the management of restrictive lung disease in SMA:5
Noninvasive ventilation using new technology
Awareness of the importance of identifying sleep-disordered breathing
New multidisciplinary approach to care
References
Wang CH et al. J Child Neurol 2007; 22: 1027–49.
Spinal Muscular Atrophy Clinical Research Center. Physical/occupational therapy. Available at: http://columbiasma.org/pt-ot.html. Accessed November 2017.
Bach JR. Paediatr Resp Rev 2008; 9: 45–50.
Lemoine TJ et al. Pediatr Crit Care Med 2012; 13: e161–e165.