SMA is a complex disorder that requires comprehensive
multidisciplinary medical care1
Comprehensive care
Effective management of SMA requires the participation of multiple disciplines and the coordination of many different aspects of care to manage the symptoms of the disease. Supportive care may include respiratory interventions, physical rehabilitation, nutritional intervention and orthopaedic support.1,2 With treatment now available for SMA, management of the disease is evolving.
Generally, a neurologist or paediatric neurologist should be in charge of coordinating assessment and appointments and monitoring disease progression.
Palliative care
The goal of palliative care is to improve quality of life and relieve stress and discomfort, and may have a role alongside active treatment.2
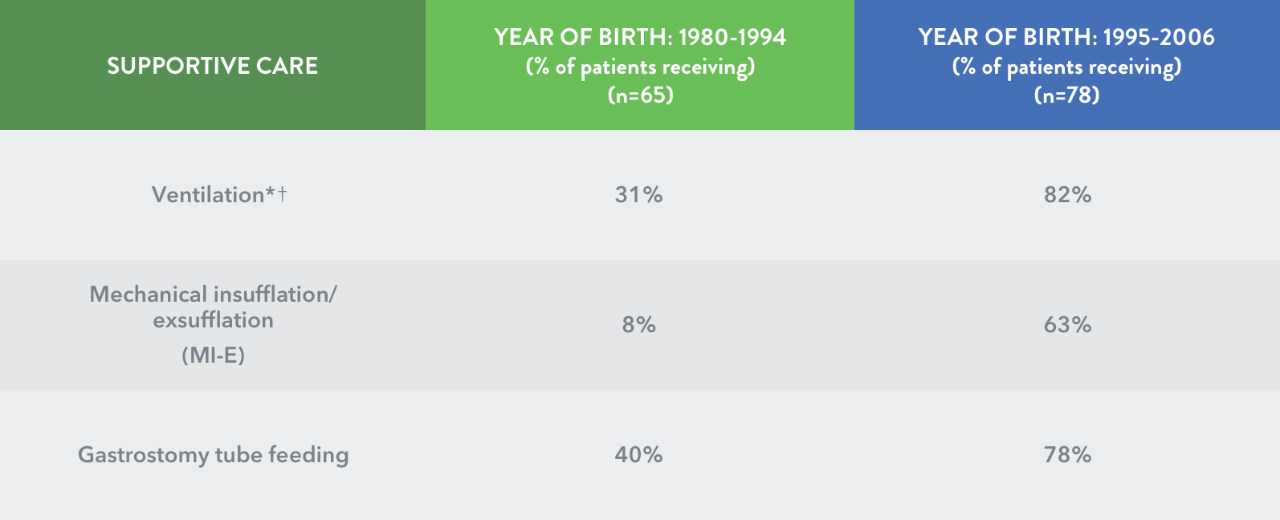
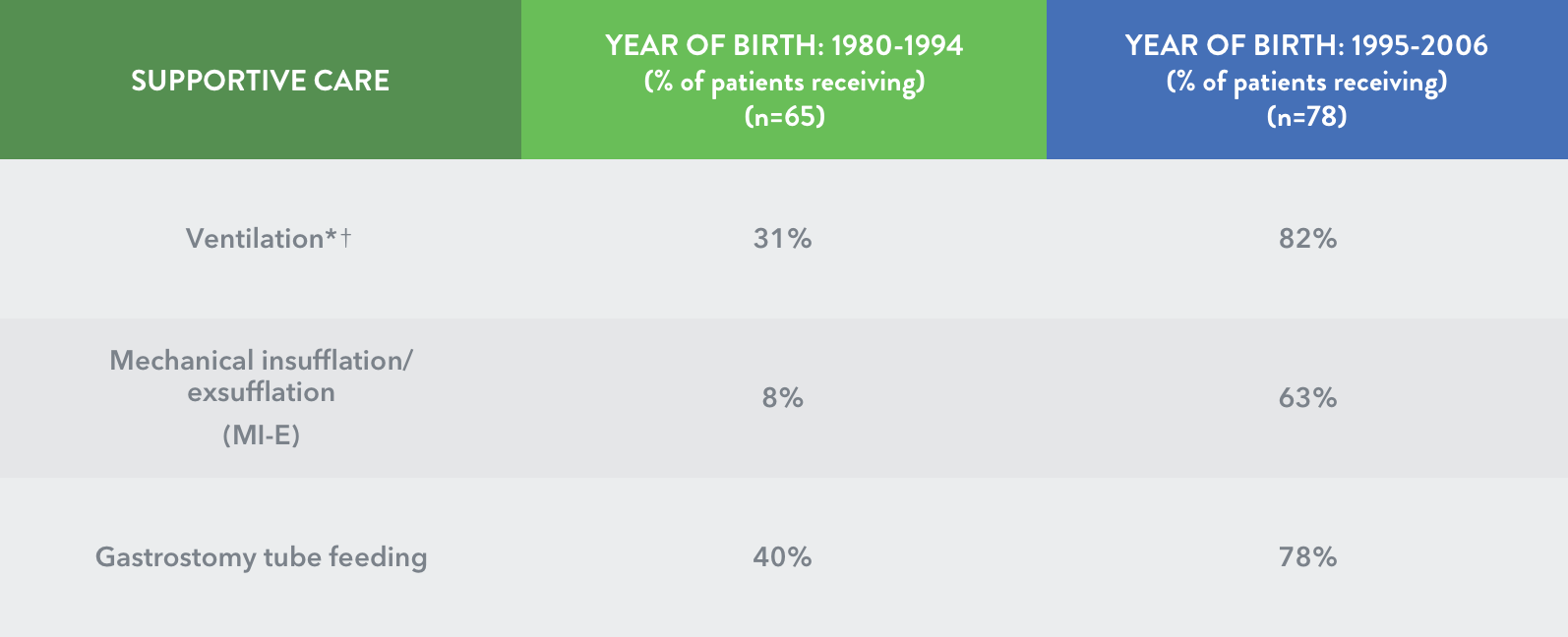
Adoption of comprehensive supportive care in infantile-onset (Type I) SMA has increased5,6
* p<0.05 for the comparison year of birth 1995-2006 vs 1980-1994. † Includes noninvasive (eg, bi-level positive airway pressure) and invasive ventilation.
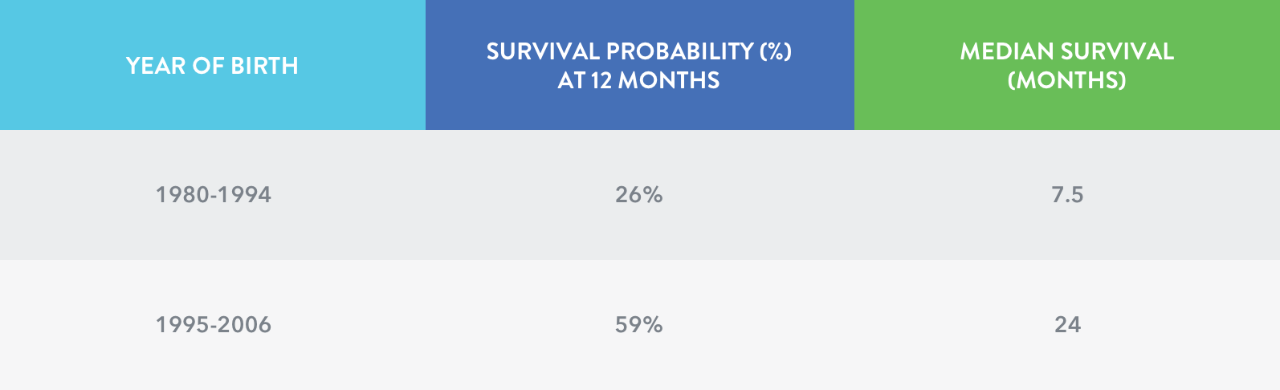
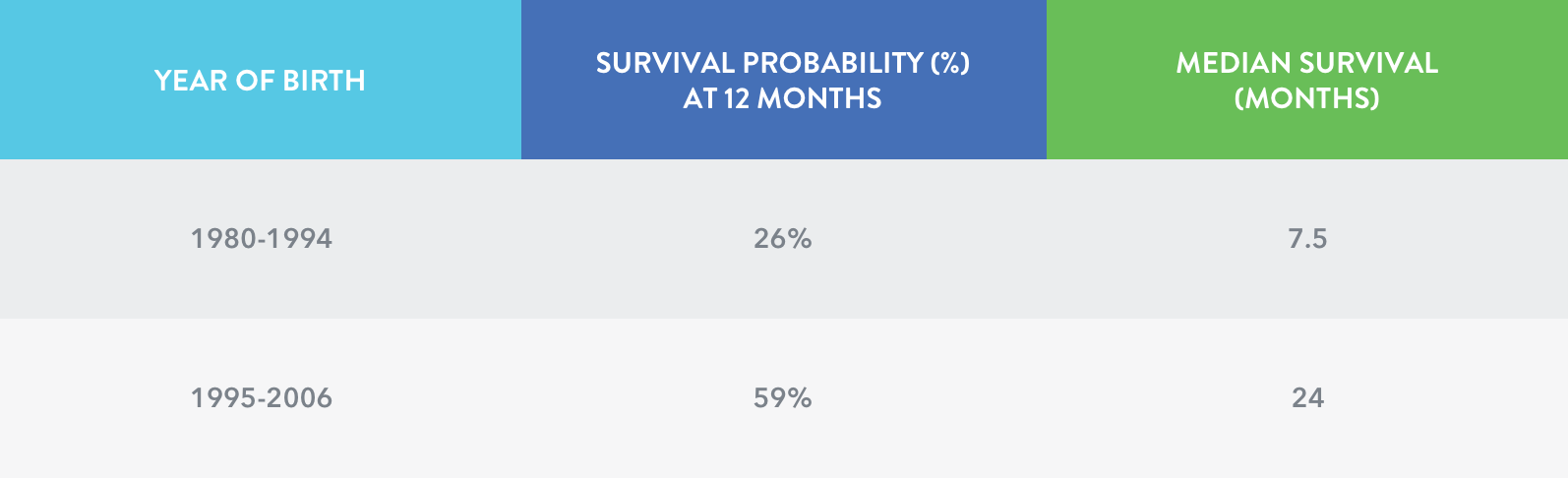
Studies have demonstrated that survival in infantile-onset (Type I) SMA has changed over time5
Survival probabilities (%) at 12 months of age based on the year of birth for death or ventilationठfor more than 16 hours per day5
‡ Kaplan-Meier method. § Includes noninvasive (eg, bi-level positive airway pressure) and invasive ventilation.
As SMA progresses, the approach to care may need to change over time1
While some individuals receive multidisciplinary care from physicians in their community, others go to a neuromuscular clinic specialising in SMA
Neuromuscular clinics specialising in SMA offer expert, coordinated multidisciplinary care
A dedicated multidisciplinary care team is the emerging paradigm at these centres
At some centres, centralised (shared) appointments allow families to see all necessary physicians on a single day at one facility
These centres provide care for the entire family, which may include genetic counselling and education
These centres may provide assistance (e.g. parking, meals, lodging) for families travelling to the centre
Advance acute-care planning is important. Consider discussing with the family appropriate responses to potentially life-threatening complications such as respiratory distress.8
Responses may include a range of interventions, from noninvasive ventilatory support to endotracheal intubation and emergency resuscitation8
Upon arriving at the emergency department, the diagnosis, current medication, respiratory status, cardiac status, and associated medical disorders should be made clear to the hospital staff8
The team involved in the respiratory care of the patient should be contacted as soon as possible8
References
Mercuri E et al.Neuromuscul Disord 2018; 28: 103–15.
Finkel RS et al.Neuromuscul Disord 2018; 28: 197–207.